Knowing the senses (If you know the anatomy of all the senses, skip this part.)
Defining Sensory Processing Disorder (SPD)
The SPD Controversy
Why OTs believe that SPD is an independent disorder?
Effects of SPD not existing in the DSM-5
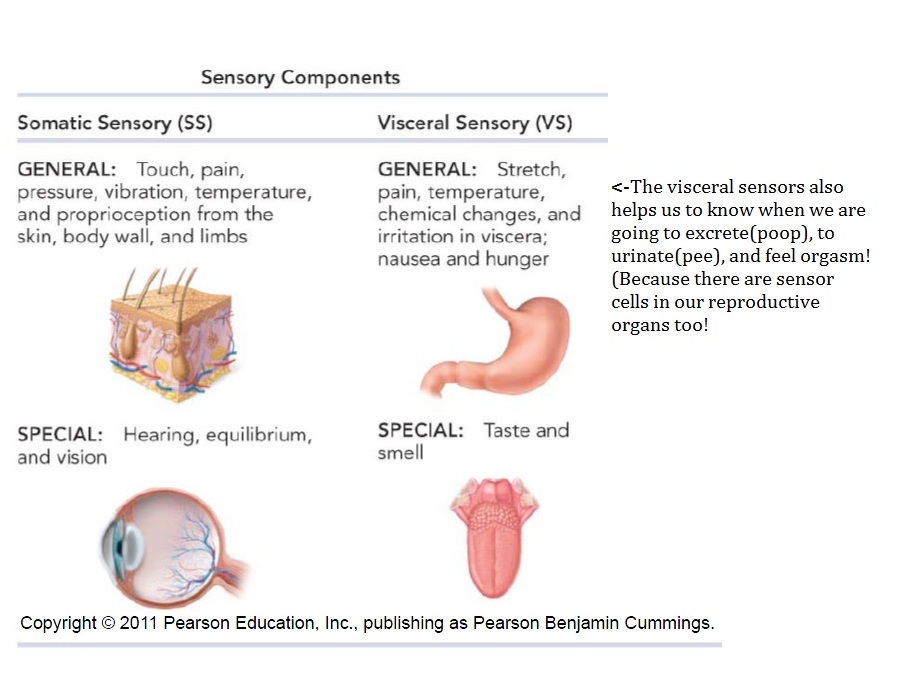
In order to fully understand Sensory Processing Disorder, I want to make sure that we know all the senses in our human bodies. First, we have more than five senses. The senses are first categorized by where the senses are detected: Does it detect stimuli in the somatic region, or around the surface of the body? Or does it detect stimuli at the visceral region, or deep in the body? After that the senses are further group into how frequently they are found in the body. Are they seen in a “specialized" location? Or “generally” around the whole body?
Balance is often called the vestibular sense because the balance receptors only exist in the semicircular canals and the vestibuleof the ear. (Ah ha!)
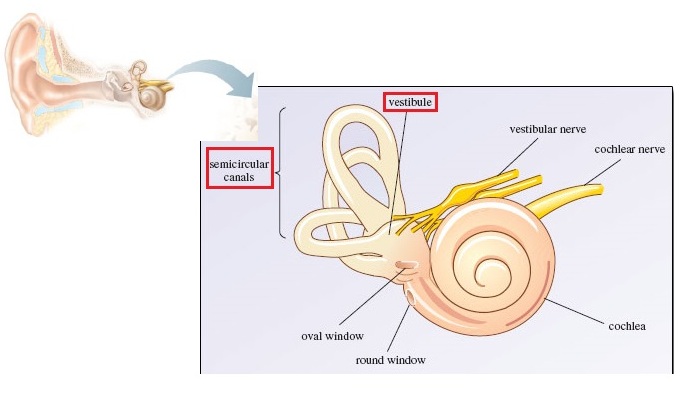
Considering that we are always moving out head even when we are seating still, the vestibule and the semicircular canals prevent us from feeling dizzy! However, it cannot always prevent us from feeling dizzy, such as after spinning for too long, or squirting water into our ear, we feel dizzy too because we are squirting directly onto our vestibule!
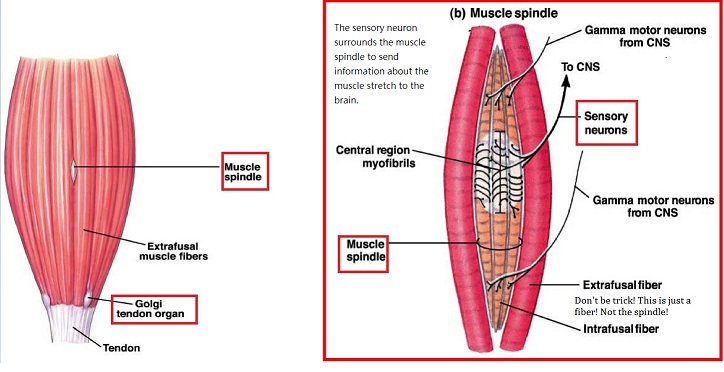
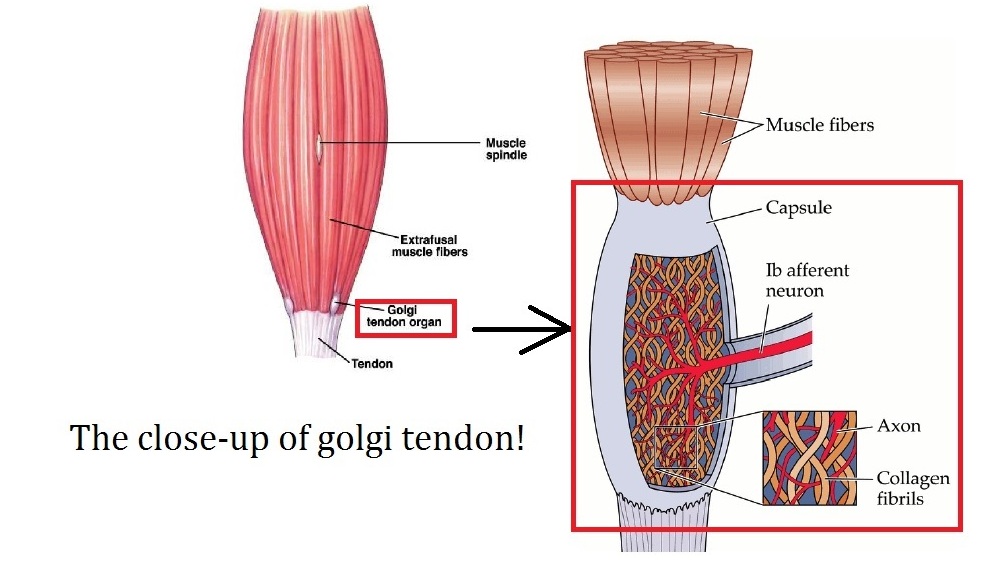
Proprioception is the ability to sense where our arms and legs are when we are both still and moving. Plus, it helps us to know which muscle, tendon and joint we are using. For example, proprioception helps some of us to type the keyboard without looking at the keyboard. Furthermore, thanks to proprioception we can do silly, but amazing things: We can close our eyes and still touch our nose! Proprioceptors, the proprioception detectors, are located in:

Considering that all of these senses go to the brain, what happen when a patient’s brain cannot interpret, or process, these stimuli appropriately? Then these patients have sensory processing disorder. However, SPD is an umbrella term for all sensory processing disorders, it is further divided into “subtypes.” Here is the chart.
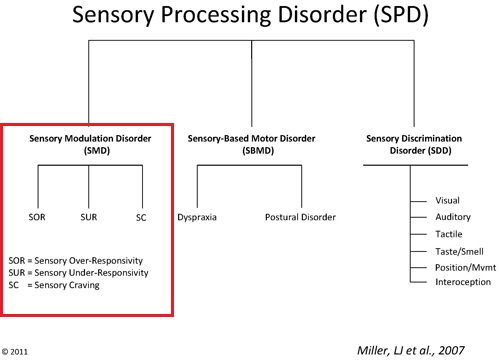
However, USUALLY, when pediatric OTs talked about SPD, they are talking about the disorders in the RED BOX because pediatric OTs treats these patients the most. So I will spend the time talking about the subtypes, Sensory Over- Responsivity, Sensory Under-Responsivity, and Sensory Craving. The table below shows the characteristic and the sensory problems that each subtype patient faces.
| Sensory Over-Responsivity | Sensory Under-Responsivity | Sensory-Craving | |
|---|---|---|---|
| Simple definition | Too Sensitive | Cannot sense/feel anything | Will do anything to get the feelings and the sensation |
| Characteristic | Anxious | Lethargic | Always on the go, so often misdiagnosed as having ADHD |
| Tactile (Touch) | You feel that your shirt tag is stabbing your back. | You cannot feel pain: You leave your hand in the boiling water without knowing that you are burning your hands! | You love to touch everything. |
| Oral(Taste) | You only want to eat Mac & Cheese because other food just tastes too bad. | “does not notice or care if foods are spicy or bland” | You like to chew on non-food objects, such as chairs. |
| Olfactory | You avoid a lot of places based on smell. | “does not notice a strong odor in the refrigerator that others instantly notice” | You love to smell everything, regardless how dangerous/poisonous it is. |
| Visual | The indoor light is too bright for you. | “Loses place when reading, complains of eyes being tired” | You want to look everywhere, and even put your hands in front of your eyes. |
| Auditory | For you, the sound of a vacuum is a bomb explosion. | You can barely hear anything, so sometimes people think you daydream often. | “Enjoy background noise” |
| Vestibular | You do not want to move because whenever you move, you feel dizzy. | “does not voluntarily choose to play on playground equipment, preferring sedentary tasks” | You love to stay on the swing, and even spinning, for an ultra-long time. |
| Proprioceptive | “may not like to feel pressure on their feet or legs, and refuses to jump, hop, or skip” | “slumps in chair or leans on walls, may have weak muscles” | You love running, crashing and jumping. |
| Visceral | You want to hold your poop as long as possible because you felt that your poop is like a cat claw scratching you whenever you poop. | “has toileting accidents, unaware of feeling hungry, poor awareness of where body is in space” | N/A |
| Source (See Information Reference) | 2 and 3td> | 3 | 4 |
It can be difficult to differentiate sensory-craving and sensory under-responsivity because at the outside, the kids can display similar symptoms. For example, both kids are shouting as they speak. However, they are shouting for different purposes: The sensory-under responsive kid shout to hear, but the sensory craving kid shout to receive their auditory stimuli.
To make diagnosing more complicated, a patient with SPD can have different kind of impairments across all of their senses: For example, a patient can crave for proprioceptive stimuli, but be under-responsive to touch, and hypersentive to hearing.
Looking at these symptoms, don’t these symptoms sounds like symptoms of autism and ADHD? When kids with autism are spoken to, they look into somewhere else, instead of establish eye contact. Most psychiatrists would say that their lack of eye contact is caused by social deficit, not by a sensory deficit. The kid who runs nonstop in the classroom: Is he craving for proprioception inputs, or does he have lack of impulse control because of ADHD? Therefore, the question is: Does SPD exists on its own or just another symptom of autism and ADHD?
Currently, the DSM-5, the bible of psychiatry, does not recognize this disorder: The DSM revisionists believe that SPD is a symptom of autism and ADHD. Furthermore, they believe that SPD needs more research to be understood. On the other hand, OTs believe SPD exists, and it is completely different from autism and ADHD.
ADHD and SPD are different because the patients with SPD:
*Although there is no current study comparing ADHD to SPD on the neurological level, the DTI (the X-ray to see the brain connection, especially the white matter) data consistently shows that ADHD has problem at the frontal lobe connection, specifically superior longitudinal fasciculus, anterior coronal radiate and fronto-strial pathways. However, a study in 2013 by Owen et al from UCSF used DTI to show that children with SPD have significantly less connections with their posterior corpus callosum, which is the portion of the brain that connects the two hemispheres.
Autism and SPD
There is neurological difference between these two disorders (Chang et al., 2014). Here is the difference in pictures:
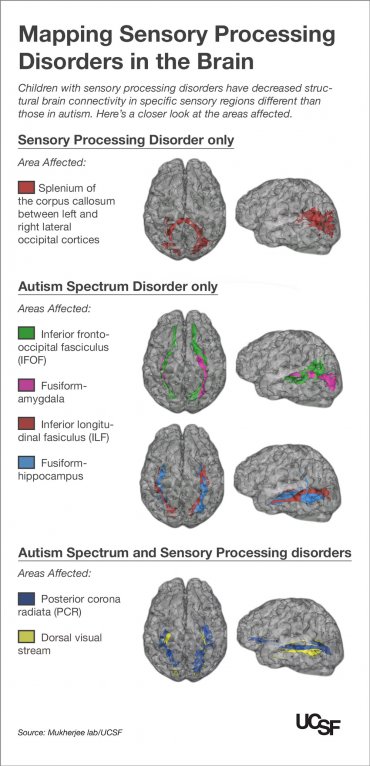
Side note: This is a study conducted by the same group of UCSF researchers who in 2013 discovered that SPD have lower connection at the posterior corpus callosum compared to healthy controls.
The article in simple English http://www.ucsf.edu/news/2014/07/116196/kids-autism-and-sensory-processing-disorders-show-differences-brain-wiring
The actual article in PDF
Information References
Figure References